Research
Brush With Confidence

Clinical studies are conducted on DentistRx products to ensure efficacy, performance and quality standards of the brand are met or exceeded. Some study highlights can be found below, with the full reports available on the sidebar.
InteliSonic Plaque Removal Evaluation
- Superior to a leading sonic toothbrush in whole mouth and gumline plaque removal
- Comparable to a leading sonic toothbrush in interproximal (between teeth) plaque removal
- Users expressed an immediate sense of clean after brushing
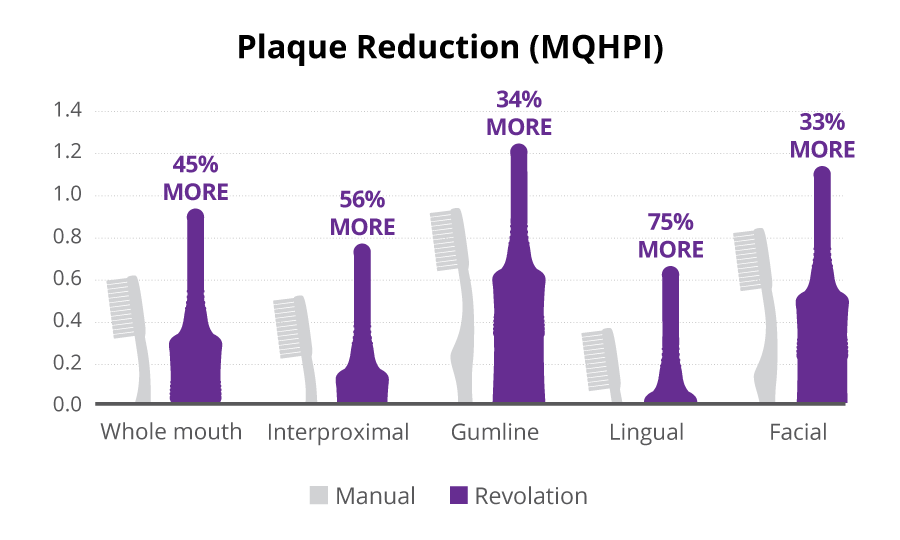
Revolation Plaque Removal Evaluation
- 75% more lingual (back of teeth) plaque removal than manual brushing*
- 56% more interproximal (between teeth) plaque removal than manual brushing*
- 45% more whole mouth plaque removal than manual brushing*
DentistRx UV Sanitizer Efficacy
- Effectively kills up to 99.9% of common bacteria and viruses (E. Coli, H. Simplex, Salmonella, Candida Albicans) from brush head surfaces
- Effectively kills up to 96.8% of the H1N1 virus from brush head surfaces

Comparison of Plaque Removal and Safety by InteliSonic® DRX-10000 and Sonicare Healthy White 700®
Goyal, C.R.; Qaqish, J.G.; Galustians, J.; McInnes, C.; BioSci Research Canada, LTD. Mississauga, Ontario; Data on file, 2010
Objectives
To evaluate and compare the plaque removal efficacy and safety of InteliSonic® DRX-10000 and Sonicare Healthy White 700® Series power toothbrushes after two minutes of brushing on normal mode for InteliSonic and clean mode for Sonicare Healthy White.
Methodology
Twenty-five subjects were enrolled in a randomized, examiner-blinded, crossover clinical study. To be enrolled into the study, subjects needed a whole mouth plaque level score of >0.60 as determined by the Refined Modified Navy Plaque Index (RMNPI). Subjects refrained from all oral hygiene (including chewing gum) for 23-25 hours prior to all study visits. The two study power toothbrushes included the InteliSonic DRX-10000 and the Sonicare Healthy White 700. InteliSonic was operated in the Normal brushing mode and Sonicare was operated in the Clean brushing mode. All toothbrushes were fully charged and Sonicare’s Easy-start® feature, which reduces bristle motion, was disabled.
At each study visit, pre-brushing plaque scores (RMNPI) were obtained and an intraoral exam, including both hard and soft tissue, was performed. Following assignment to the randomized treatment, subjects were asked to brush for 2 minutes with their assigned toothbrush and toothpaste according to the respective toothbrush manufacturer’s brushing instructions. A post-brushing plaque assessment (RMNPI) was performed. Product safety in the oral cavity was also assessed. Subjects returned in approximately 48 hours for the crossover visit. Subjects also completed a product evaluation and questionnaire at each visit. Plaque score data was analyzed for whole mouth, interproximal, and gumline plaque removal for each study toothbrush. The significance of the mean change in the plaque score was made within treatment groups using paired t-tests. To evaluate comparisons between treatments, repeated measures analysis of variance (ANOVA) was used for the plaque change scores.
Results
Both toothbrushes showed statistically significant plaque reduction (whole mouth, interproximal and gumline) from pre-brushing (p<0.001). InteliSonic removed significantly more whole mouth plaque than Sonicare with a 78.9% plaque reduction for InteliSonic compared to 75.0% for Sonicare (p=0.042). InteliSonic also removed significantly more gumline plaque, 73.9% for InteliSonic compared to 68.3% for Sonicare (p=0.024). Interproximal plaque reduction for InteliSonic removed was 84.8% versus 83.2% for Sonicare, with this difference not being statistically significant (p=0.356). Both toothbrushes were safe to use; no adverse events were reported. Based on responses to the questionnaire, both toothbrushes were well accepted and received positive evaluations in the areas of cleaning, gentleness, and comfort. Positive comments on InteliSonic included an overall feeling of clean and gentle bristles.

Conclusions
- InteliSonic was effective in removing plaque from whole mouth, gumline and interproximal surfaces.
- InteliSonic was superior to Sonicare for whole mouth and gumline plaque removal.
- InteliSonic and Sonicare achieved comparable interproximal plaque removal.
- Both brushes were found safe for everyday use.
- No adverse events reported.
- Subjects using InteliSonic expressed an immediate sense of clean after brushing.

Comparison of Revolation DRX-9000 and a Manual Toothbrush for Plaque Removal and Safety
Kleber, C.J.; Milleman, K.R.; McInnes C. University Park Research Center, Fort Wayne, In and DentistRx, Redmond, WA
Objectives
To evaluate and compare the plaque removal efficacy and safety of Revolation™ DRX-9000 and a manual toothbrush during typical use.
Methodology
Twenty five subjects were enrolled in a randomized, examiner-blind, crossover clinical study. To be enrolled in the study, subjects needed a full-mouth plaque score of = 2.00 as determined by the Modified Quigley-Hein Plaque Index (MQHPI). Subjects refrained from all oral hygiene for 24±2 hours prior to all study visits. The study consisted of one clinic visit for each test product. the two test products were the Revolation™ power toothbrush (Dentistrx®, Redmond, WA) and a manual toothbrush (Oral-B® Indicator®, Soft 35 Compact, Procter & Gamble, Cincinnati, OH). Subjects brushed for two minutes with the Revolation as recommended by the user’s manual. To provide a typical Revolation tooth brushing experience, subjects brushed the complete dentition for 1 minute with the everyday brush head and subsequently for 1 minute with the perio brush head. To provide a typical manual toothbrush brushing experience, subjects brushed the complete dentition for 1 minute. All subjects were given verbal cues every 15 seconds to move to the next quadrant, thereby equalizing brushing throughout the mouth.
At each study visit pre-brushing plaque scores (MQHPI) were recorded along with data from an intraoral exam of soft and hard tissue. Subjects were then randomly assigned to treatment and given written and oral brushing instructions according to their assignment. Subjects brushed in the presence of an assistant who provided verbal cues when to move between quadrants of the oral cavity. A post-brushing assessment of plaque removal and tissue was performed as was done prior to brushing. At the end of the visit, subjects completed a written questionnaire. Subjects returned approximately 48 hours for the crossover visit wherein the alternate treatment was assigned. Plaque score data was analyzed for the whole mouth as well as for interproximal, marginal (gumline), facial, and lingual regions. The significance of the mean change in the plaque score was made within treatments using paired t-tests. To evaluate comparisons between treatments, repeated measures analysis of variance (anova) was used for the plaque change scores.
Results
Analysis of the pre-brushing plaque scores indicate that both groups (Revolation and manual) were balanced at baseline. Both toothbrushes showed statistically significant reductions in plaque after brushing (p<0.0001) for the full mouth plaque scores as well as scores for the various regions of the oral cavity. The Revolation toothbrush was significantly more effective than the manual toothbrush in removing plaque for all the various tooth surfaces (p<0.0001). The results indicate that both brushes performed the best on easier to reach plaque along the gumline and on the facial surfaces. The difference in mqhp scores between Revolation and a manual toothbrush, expressed on a percentage basis, was greatest in the interproximal and lingual regions. The Revolation was particularly more effective in removing plaque in these hard-to-reach areas. Both toothbrushes were found safe to use, and no adverse events were reported. Based on responses to the questionnaire, subjects felt both brushes were effective in removing plaque, but that Revolation provided a more gentle cleaning experience.
Conclusions
The results of this clinical study found:
- Revolation was significantly more effective than a manual toothbrush in removing dental plaque.
- Revolation was particularly more effective at removing hard-to-reach plaque in the Reduction in Plaque (MQHPI) interproximal and lingual areas.
- Both brushes were found to be safe on gums, teeth, and restorations.
- No adverse events were reported.
- Subjects reported that Revolation produced a gentle cleaning action.
Oral-B® and Indicator® are registered trademarks of the Procter & Gamble Company
Evaluation of Sanitization Efficacy by DentistRx® UV Sanitizer
Mai, T; Microbiotest, A Division of Mircobac Laboratories, SGS-CSTC Standards Technical Services Co., Ltd.; Data on file, 2008, 2010
Objectives
To evaluate, in vitro, the virucidal, bactericidal and fungicidal efficacy of the DentistRx ultraviolet (UV) toothbrush sanitizer on specific microorganisms.
Methodology
Several in vitro studies were conducted to evaluate the efficacy of the UV sanitizer. For in vitro testing of Human Influenza A Virus (H1N1) and Herpes Simplex Virus Type 1, the ultraviolet sanitization device was tested for their viral contamination reduction capacity. Each brush head was contaminated using the selected virus, dried under room temperature in a bio-safety cabinet, and then subjected to the ultraviolet treatment for 7 minutes. After treatment, the toothbrush was transferred to a tube containing extraction medium and vortexed. The extracted sample was serially diluted and assayed for presence of survived infectious virus. All of the procedures involved in performance of this study were followed according to GLP regulations.
For in vitro testing of Escherichia coli (E. Coli), Salmonella and Candida Albicans bacteria and fungus, each culture suspension was inoculated on a sterile test surface measuring 2.0 x 5.0 cm2. The bacteria had to reach a quantity of 1x106~5x108 cfu/mL prior to testing. At a distance of 0.5 cm, the cultures were then exposed the ultraviolet light for 7 minutes. At the end of the ultraviolet light exposure, bacterial counts were measured to evaluate bactericidal effectiveness using the formula (To-Tn)/Tx100%, where To is equal to the viable bacteria count of the positive control sample, Tn is equal to the viable bacteria count after 420 seconds of reaction (UV exposure time) and n is equal to the reaction time.
Results
The DentistRx UV Sanitizer is effective in eliminating 99.9% of E.Coli, Salmonella, Candida Albicans and Herpes Simplex and 96.8% of the H1N1 virus.

Conclusions
The DentistRx UV Sanitizer effectively kills up to 99.9% of common bacteria and viruses and up to 96.8% of the H1N1 virus from the brush head surfaces.